MP1130 - Abdomen with bilateral Hernias

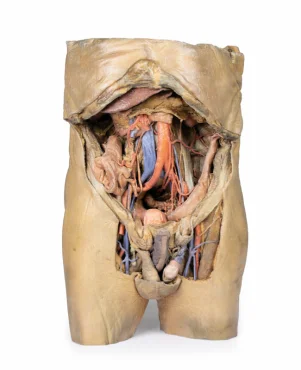





This 3D model represents one of the largest and most complex in the series, consisting of a partial torso from the diaphragm to the proximal thigh with a complete abdominal cavity preserving varying levels of dissection. This 3D model also records the rare, simultaneous occurrence of indirect and direct inguinal hernias allowing for a consideration of the anatomical underpinnings for both conditions. Given the scale of the dissection this 3D model description is divided into discrete parts based on views and regions.
The diaphragm
On the superior aspect of the model the diaphragm is preserved, and while slightly distorted due to removal of the thoracic ribs through dissection, both domes and costodiaphragmatic recesses can be appreciated. The fibrous pericardium is present on the superior surface of the central tendon, with the terminal part of the inferior vena cava visible in the caval foramen. Just lateral to caval foramen is the oesophagus within the oesophageal hiatus, and then the descending thoracic aorta approaching the aortic hiatus just ventral to the thoracic vertebrae.
The epigastric and hypochondriac regions
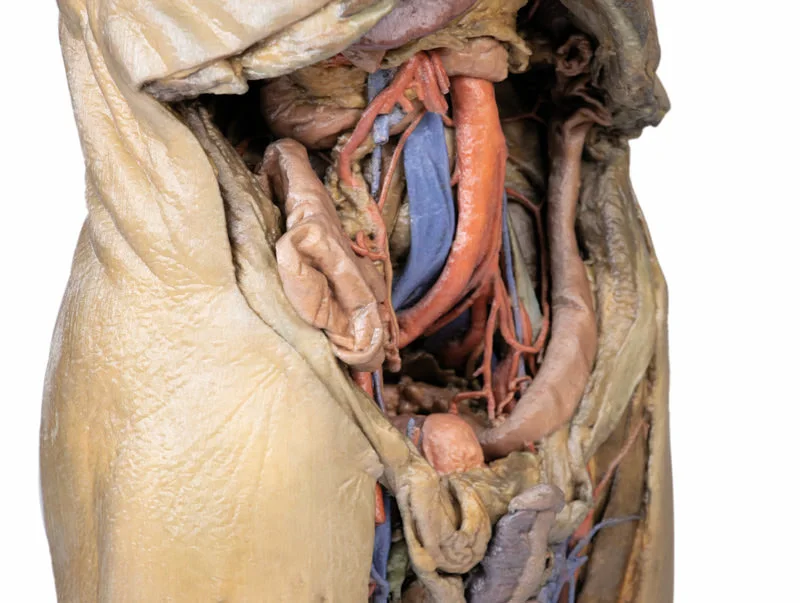
Within the abdomen, the anterior abdominal wall, greater omentum, and much of the gastrointestinal tract has been removed alongside the parietal peritoneum over the posterior abdominal wall to expose retroperitoneal organs and structures. In the superior abdomen, the terminal portion of the oesophagus has been retained and can be seen entering the cavity just lateral to the left lobe of the liver. The removal of the stomach has exposed the extent of the pancreas from the head (positioned within the arc of the duodenum) to the tail extending to the capsule of the spleen preserved in the left hypochondrium. Superior to the pancreas, the splenic artery and common hepatic arteries can just be observed spanning across the narrow space between the pancreas, diaphragm and liver. The splenic follows its archetypical “tortuous route” towards the spleen, and strongly divides prior to reaching the hilum (and adjacent to the splenic vein). The common hepatic can be seen dividing into the gastroduodenal (visible again as a cut vessel just inferior to the duodenum) and giving off the right gastric artery; these vessels lie superficial relative to the hepatic portal vein. The superior mesenteric artery and vein can be seen passing anteriorly near the head of the pancreas and horizontal part of the duodenum, and the retained ileocolic artery can be traced to the caecum of the large intestine in the lower right quadrant of the abdomen. The inferior mesenteric vein can be, in part, appreciated arising from the retained superior rectal vein ascending from the undissected true pelvis and spanning across the superficial aspect of the descending thoracic aorta.
Inferior to the liver the gallbladder can be viewed just between the right and left anatomical lobes. On the left, the passage of the renal artery and vein can be seen just deep to the pancreas, and the ureters can be observed descending from the partially exposed kidney across the superficial surface of the exposed psoas major and minor muscles.
The umbilical and lumbar regions
Most of the organs occupying the umbilical and lumbar regions of the abdomen have been removed in order to expose structures in the posterior abdominal wall. In the midline, the descending abdominal aorta and inferior vena cava dominate the region, with the testicular arteries and veins isolated and traceable towards the inguinal regions. Two right lumbar arteries are visible arising from the aorta, and despite removal of the mesenteries and most of the colon the inferior mesenteric artery can be seen giving rise to the left colic, sigmoid and superior rectal arteries. On the right side of the specimen inferior to the kidney, the subcostal, iliohypogastric and ilioingual nerves are exposed alongside the circumflex iliac artery.
The hypogastrium and iliac regions
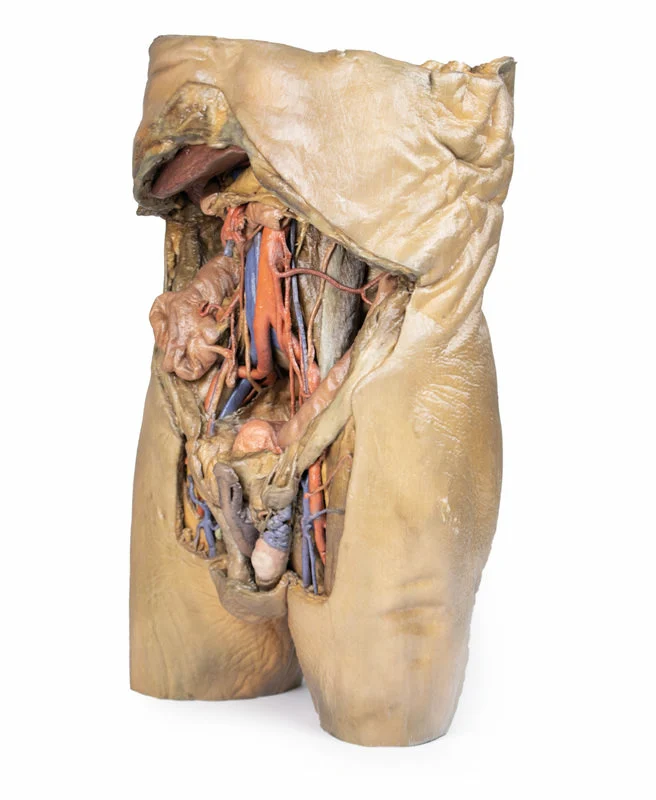
In the midline, the bifurcation of the descending abdominal aorta into the common iliacs (and subsequent division into the internal and external iliacs) can be observed deep to some of the overlying structures (e.g., testicular vessels, ureters) noted previously. On the right side, the obturator artery can be seen traversing from its origin towards the anterior aspect of the pelvis. The mirrored merging of external, internal and common iliac veins into the inferior vena cava is also preserved. Within the confines of the true pelvis the peritoneum has been retained over the region, covering the urinary bladder adjacent to the pubic symphysis and obscuring the rectum as it descends from the sigmoid colon. In the right iliac region the very terminal part of the ileum and caecum with appendix fill the iliac fossa, with the appendix (and appendicular artery) visible just superficial to the testicular artery, vein and genital branch of the genitofemoral nerve descending towards the inguinal canal. In the left region, the sigmoid colon descends across the iliac fossa. As it approaches the anterior abdominal wall, an epiploic appendage contribution to the indirect hernia can be observed just lateral to the retained inferior epigastric artery.
The inguinal region and perineum
A distinctive and unique feature of this model is the dissection of simultaneous direct and indirect hernias preserved on the right and left sides, respectively. While most of the anterior abdominal wall has been removed, the inferior epigastric arteries (and accompanying veins) have been retained to allow for interpretation of the herniations. On the right side, a distinct outpouching of the parietal peritoneum has formed medial relative to the inferior epigastric artery, representing an indirect herniation event. On the left side, the hernia sac extends laterally relative to the inferior epigastric artery and into the opened spermatic cord, with continuity of the epiploic appendage from the sigmoid colon into the sac.
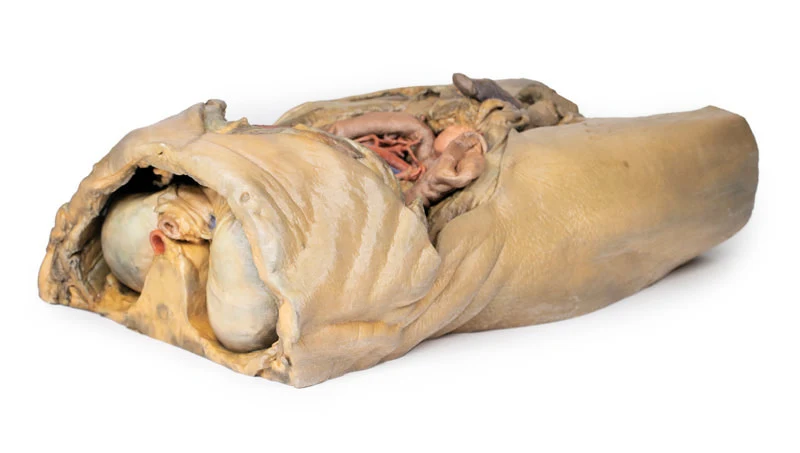
The skin over the perineum has been removed in order to demonstrate both the structure of the penis (with both the corpus spongiosum and corpora cavernosa contrasted) and the position of the testes and spermatic cords relative to the anterior abdominal wall. On the right side, which in this individual is impacted by a direct hernia, the spermatic cord has been left undissected allowing for an appreciation of the external spermatic fascia from the inguinal region through to the testis. On the left side, the spermatic cord has been opened and is dominated by the enlarged and varicose testicular vein (reflecting the impact of the indirect hernia exposed within the cord) just superior to the epididymis and exposed tunica albuginea of the testis.
The thigh
Anterior dissections into the femoral triangle region have been undertaken to both thighs with varying preservation of contents. On the right side the femoral sheath has been removed to expose the femoral artery, vein and the deep inguinal lymph nodes. The femoral artery has been sectioned with a portion removed to expose the origin of the profunda femoris and to better appreciate the draining of the great saphenous vein into the femoral vein. Just lateral to these structures the very terminal component of the femoral nerve is visible. On the left side a slightly larger dissection window has been opened to expose more of the underlying anterior and medial thigh compartment muscles, from the sartorius and iliopsoas laterally to the pectineus and adductor longus medially. The femoral artery has been preserved, with a well-preserved superficial circumflex iliac artery and the origin of the profunda femoris visible adjacent to the femoral nerve.
The model terminates at the level of the mid-thigh, and while not a primary focus of the model the spatial organisation of structures in the cross-section can be seen. This includes the anteriorly positioned femoral diaphysis with tightly-packed anterior compartment muscles and the passage of the femoral artery and vein in the subsartorial canal.
- Quantitative unit
- ks

MP1130 - Abdomen with bilateral Hernias


